
Types of movements
- Unintentional – involuntary
- Intentional – voluntary
Purpose of movements
- Protection/maintenance of posture
- To execute a voluntary movement in response to a thought/ idea or external stimulus [ from eyes, ears, touch, etc]
Posture provides background for movement
Movement starts with one posture and ends with another
Coordination before and after movement
- Initiation & coordination of movement is carried out by a complex system of
- hierarchical control
- feedbacks
- continuous adjustment
- Eg. Walking
- left upper limb coordinated with right lower limb
- smooth & balanced
- left upper limb coordinated with right lower limb
Servo systems
- No control system
- Feedforward system
- Feedback system


Scheme of motor movement

- Idea
- eg. i want to touch my toes
- Planning & programming
- Cerebral cortex (Cortical association areas)
- plans and execute movement
- Basal ganglia
- initiates movement
- Lateral cerebellum
- refines movement
- Cerebral cortex (Cortical association areas)
- Thalamus
- Premotor & motor cortex
- Pyramidal system
- to corticospinal tract
- Extrapyramidal system
- Rubospinal
- Reticulospinal
- Tectospinal
- Vestibulospinal
- Pyramidal system
- Alpha motor neuron (lower motor neuron)
- final common pathway
- Execution
- muscles
- Monitoring
- intermediate cerebellum
- Feedback
- back to premotor & motor cortex





_____________________________________________________________________
The basal ganglia
Responsible for planning and programming of movements.
Disorders of movements
- Hyperkinetic
- Chorea
- Huntington’s chorea
- Athetosis
- slow and writhing
- like a snake dance
- Ballism
- ballistic!
- hemiballism
- resulting from the destruction of subthalamic nuclei on the same side
- Chorea
- Hypokinetic
- Akinesia
- inability to initiate movement due to difficulty selecting and/or activating motor programs in the central nervous system
- Bradykinesia
- slowness of movement and has been linked to Parkinson’s disease and other disorders of the basal ganglia
- Akinesia
Related structures of basal ganglia

- Corpus striatum
- Striatum (neostriatum)
- caudate nucleus
- putamen
- nucleus accumbens
- Globus pallidus (pallidum/paleopallidum)
- medial (internal) segment
- lateral (external) segment
- ventral pallidum
- Striatum (neostriatum)
- Substantia nigra
- pars compacta
- pars reticularis
- Subthalamic nuclei
- Ventral tegmental area
Different pathways
- Nigrostriatal dopaminergic pathway
- dopamine releasing neurones going from Substatia nigra to the putamen (striatum)
- degeneration of this pathway –> Parkinsonism
- Intrastriatal cholinergic system
- loss in Huntington’s disease
- GABA-ergic neurons from striatum to globus pallidus (external) and Substantia Nigra
- loss in Huntington’s disease
Parkinsonism
- disorder of the extrapyramidal system, that is, the motor structures in the basal ganglia
- may be caused by degeneration of dopamine-producing cells in the substantia nigra, resulting in decreased levels of dopamine in the striatum
- Pathogenesis
- loss of dopamine and dopamine receptors
- normal aging process
- however accelerated in Parkinson’s disease
- loss of balance between cholinergic (exci
tatory) and dopaminergic (inhibitory) discharge
- loss of dopamine and dopamine receptors


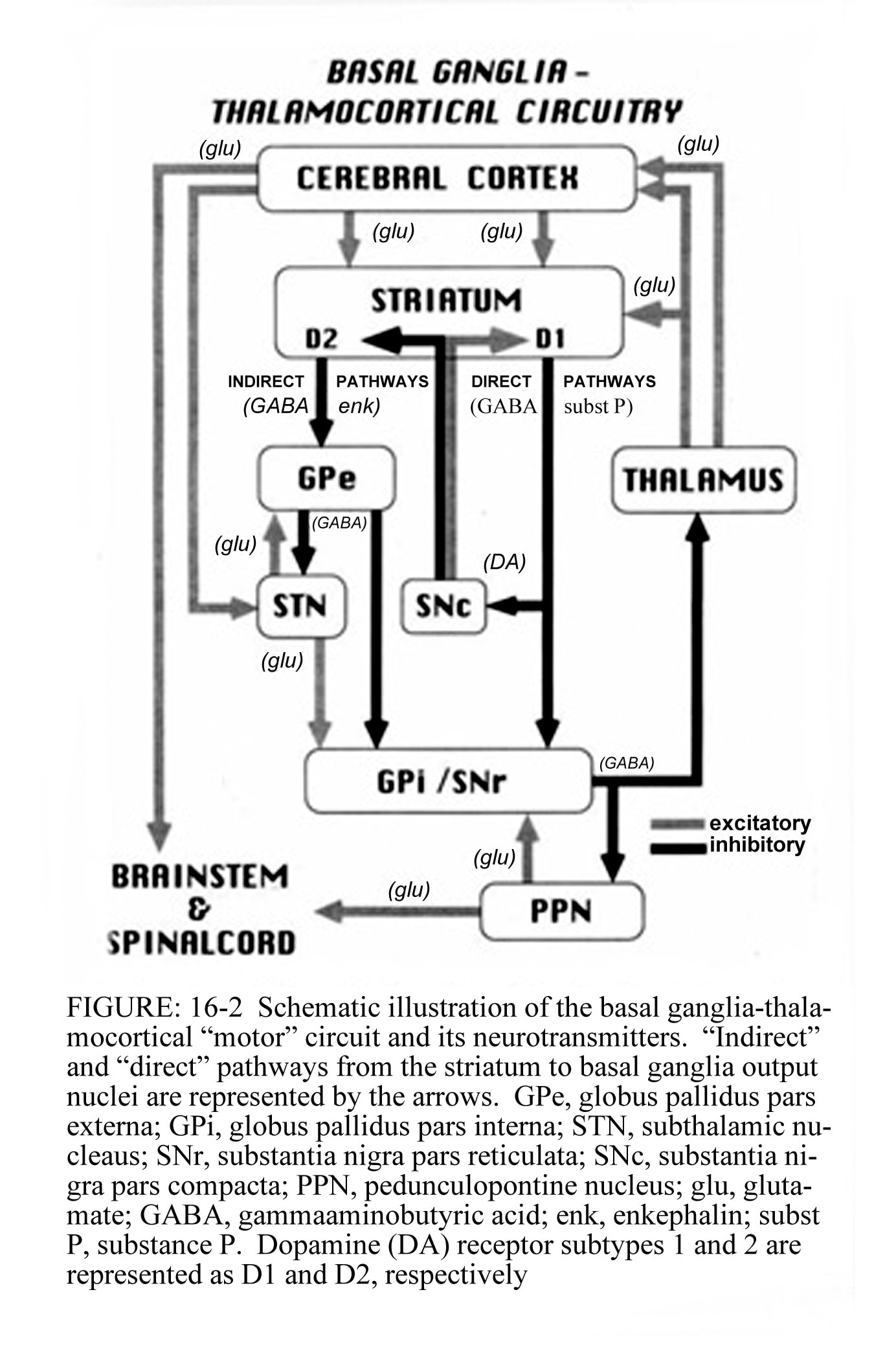
Pathophysiology of Parkinsonism
Refer diagrams above
Normally,
- The cerebral cortex plans and programs the movement
- Then signals the striatum to secrete dopamine (1 and 2)
- 2 pathways
- Direct pathway
- cortex→striatum→GPi→thalamus→cortex
- outflow from striatum
- Secrete D1
- directly inhibits GPi and Substantia nigra (SNr)
- GPi usually inhibits thalamus
- So if GPi is inhibited, so there is no longer inhibition of the thalamus (disinhibition) –> stimulate thalamus
- sends inhibitory output to the ventral lateral (VL) nucleus of the thalamus
- stimulate THALAMUS
- excites cortex
- initiate movement
- In parkinson’s: opposite of everything
- Difficulty in initiating movement
- Indirect pathway
- cortex→striatum→GPe→STN→GPi→thalamus→cortex
- inhibit GPe and Subthalamic nucleus
- excites GPi
- further inhibit the thalamus
- inhibit thalamus
- does not excite cortex
- supresses involuntary movement
- In parkinson’s: opposite of everything
- Increases involuntary movement
- Direct pathway
Clinical features of Parkinson’s disease
- Hypokinetic features (pallidectomy is beneficial)
- akinesia
- difficulty in initiating movements
- bradykinesia
- slow performance of voluntary movement
- eg shuffling gait
- hypokinesia
- difficulty in initiating continuous movement
- inability to execute simultaneous movement
- Hypomimia/ defective kinetic automatism / masked facies
- loss of associated movements
- eg facial expressions, unconscious movements (swinging of arms), gestures, fidgety actions
- festinating gait
- bends lightly forward and walks with short quite step
- swallowing & speaking difficulties
- akinesia
- Hyperkinetic features
- rigidity
- cogwheel rigidity
- tremor at rest
- pin-rolling tremor
- loss of braking action
- can’t stop himself when pushed
- rigidity
Test for Parkinsonism
- Observe
- masked facies (loss of facial expression)
- loss of associated movements (swinging of arms when walking)
- shuffling gait
- pin-rolling movements
- Test for rigidity
- lead pipe rigidity/ cogwheel rigidity
- Push him
- can he brake himself?
- be sure to have someone catch him when he falls
_____________________________________________________________________
Cerebellum
- Planning execution of movement
- Learning of skilled motor tasks
- Receives afferent from:
- labyrinths
- through vestibulocerebellar pathway
- to maintain balance
- Proprioceptors and enteroceptors
- through spinocerebellar pathway
- postural control
- feedback during movement
- Proprioceptors from head and neck
- through cuneocerebellar pathway
- Proprioceptors from whole body
- through olivocerebellar pathway
- Ear and eye
- through tectocerebellar pathway
- Cerebral cortex
- through pontocerebellar pathway
- labyrinths
- -> goes to spinocerebellum
- medial and lateral descending systems
- Sends efferents to:
- lateral cerebellum (cerebrocerebellum)
- motor & premotor cortex
- motor planning
- vesticular nuclei
- balance & eye movements
- motor & premotor cortex
- vesticulocerebellum
- diving
- lateral cerebellum (cerebrocerebellum)
Cerebellar dysfunction
- May show no abnormality at rest
- Ataxia (with movement)
- errors in rate, force, range and direction in movement
- Defect in skilled movement
- slurred/scanned speech
- Dysmetria (past-pointing)
- Intentional tremors
- due to overcorrection
- Adiadochokinesia
- an inability to perform rapidly alternating movements, such as pronation and supination or flexion and extension
- Decomposition of movement
- movements dissected like a puppet
Tests for cerebellar dysfunction
- Speak to the patient
- slurring of speech?
- Observe
- intentional tremors
- Walk to straight line
- ataxia
- Finger-nose test
- past-pointing to the ear
- Supinate and pronate hands quickly
- adiodochokinesia
- heel-to-knee (or to shin) test
- heel cannot slide down shin in a straight line
Differentiating atax
ia – sensory or motor.
- Rhomberg’s test
- stand with feet together, hands at the side
- Sensory ataxia
- eyes open – steady
- eyes closed – unsteady
- Motor ataxia
- eyes open – unsteady
- eyes closed – unsteady
- (RHOMBERG’S SIGN +VE)